
Introduction
It should go without saying that none of us want to give our kids medication unless it is necessary. We always like to see if there are some natural remedies that can do the trick. Many low-grade fevers don’t need medication at all. Cool compresses, light clothing, fluids, and comfort might be enough. Of course there will be times that we need to move to plan B and break out the standard over the counter fever medications (antipyretics).

When to give an antipyretic
Antipyretics are medications, like Tylenol (acetaminophen) or Advil/Motrin (ibuprofen). They lower fevers and treat pain, and ibuprofen sometimes decreases inflammation. That’s basically it. So if your child is not in pain, does not have a fever, and is not inflamed, you don’t need to give it. We’ll talk later about how to think about these medications with shots.
Acetaminophen
Liquid
Acetaminophen is most often found under the brand name Tylenol. Acetaminophen is usually given every 4-6 hours. Too much Tylenol can be toxic to the liver, so it is important not to exceed the recommended dose. Do not give more than 5 doses in 24 hours.
It’s worth mentioning - acetaminophen is a bit more forgiving than ibuprofen. What matters most is the total amount over 24 hours, so you don’t need to stress about hitting every dose perfectly on schedule, as long as you’re staying within the recommended daily limit.
The only difference between infant and children’s Tylenol is that the infants packaging comes with a handy syringe for accurate dosing. Otherwise they are the same concentration of 160mg/ 5 ml (1 teaspoon). We like the “dye-free” formulations.
Suppository
This is very useful if you have a child who is vomiting, or simply hates taking meds. Even though a rectal medication feels intrusive to parents, most kids don’t tend to mind them at all.
Pro tip: keep them stored in a cool place, refrigerator fine. Giving a mushy suppository is very difficult.
Gummy
Some reluctant medicine takers will eagerly accept a gummy.
Pro tip: watch to make sure they chew and swallow. There are absolutely kids who stash a partially eaten gummy under the couch.
Powder
These quick dissolve powders are often a great choice. They can also be mixed with a spoonful of yogurt or applesauce and are a good option for fussy kids.
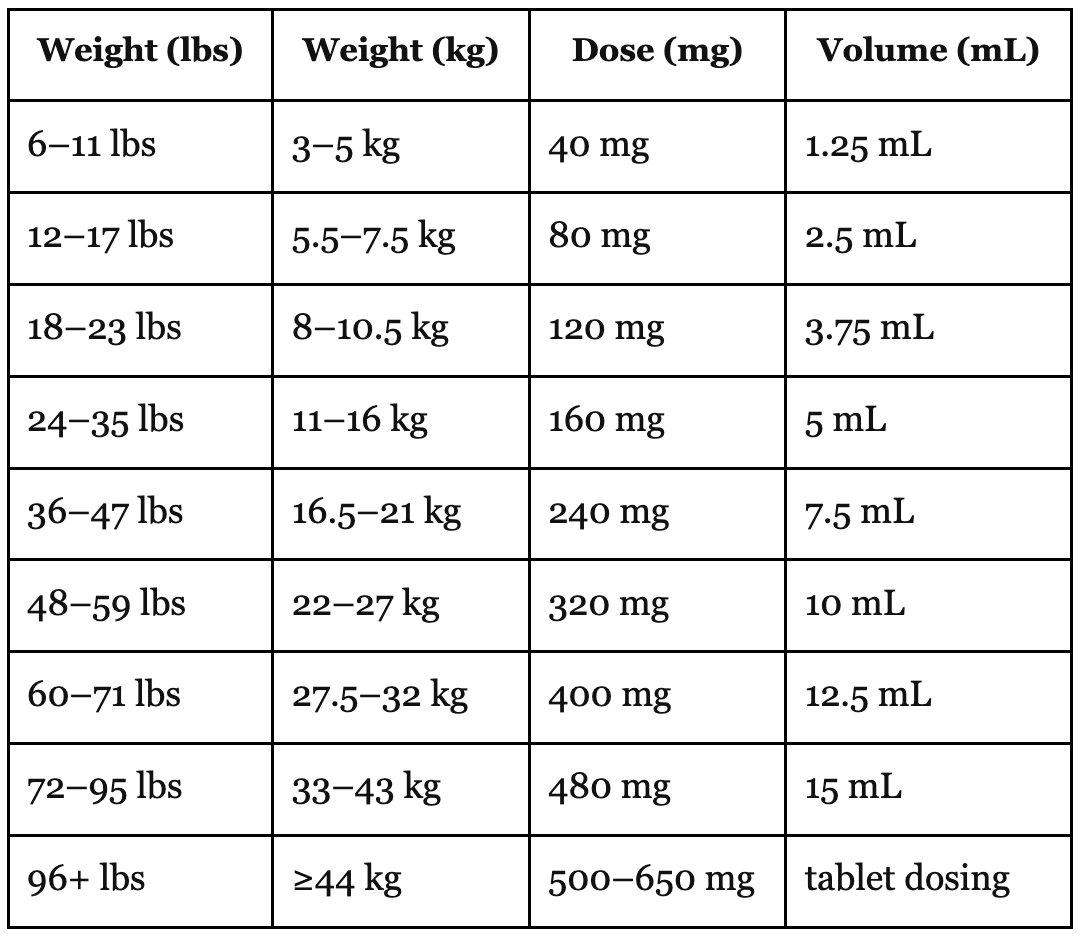
Acetaminophen Dosing Chart
Ibuprofen
Ibuprofen may be sold under the brand names Motrin or Advil but generic brands are acceptable. Ibuprofen is generally not recommended before 6 months unless cleared by a clinician.
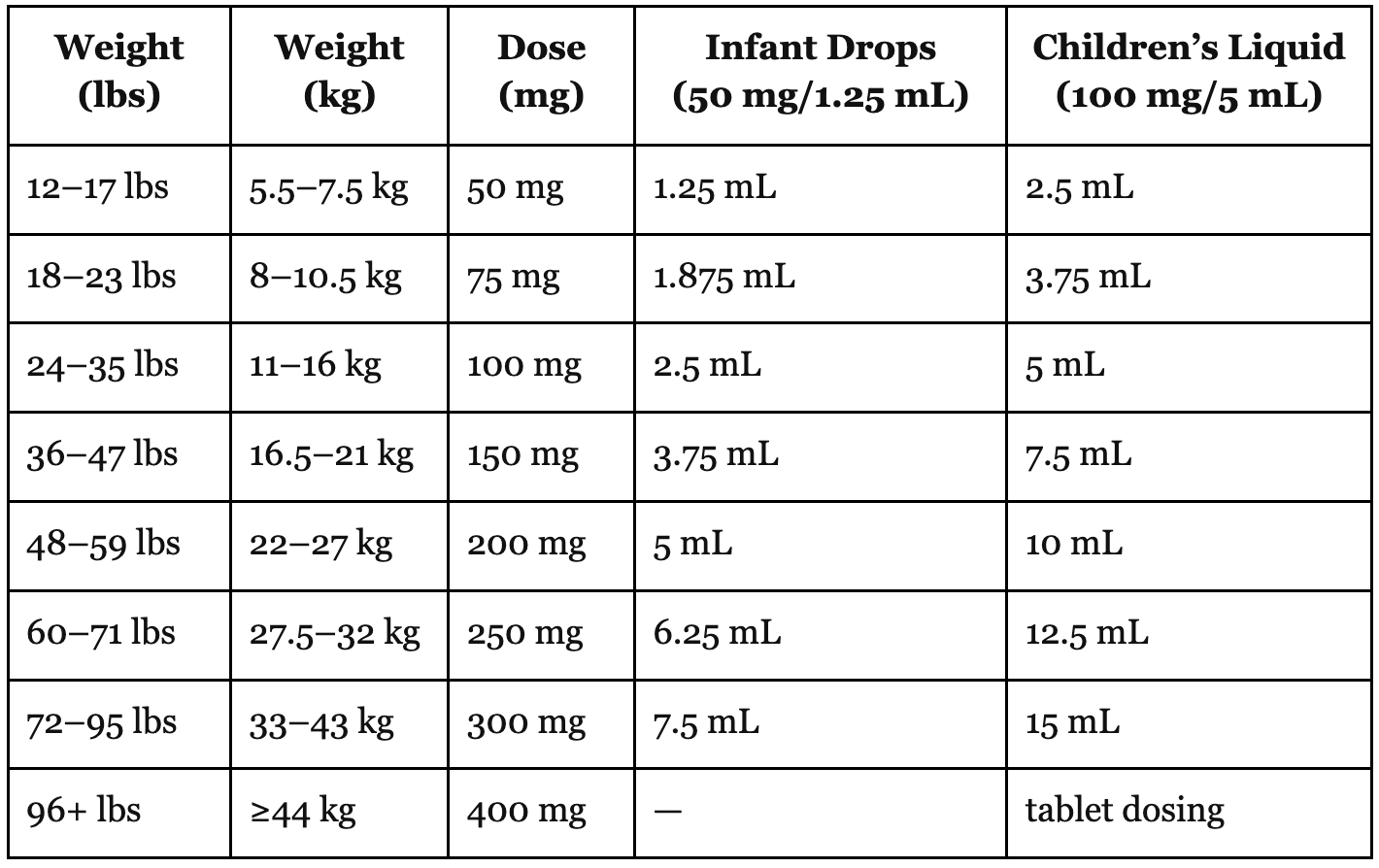
Ibuprofen has a double concentrated infant version:
The infant version is 50 mg/1.25 ml
The children’s version is 100 mg/ 5 ml
It is very important to make sure you pay attention to which one you are using.
Ibuprofen is usually given every 6-8 hours.
Ibuprofen Dosing Chart
The correct dose adjusts with your child’s weight. That dose that the doctor calculated for you when your infant came in for their first shots? It is not going to cut it for your 25 pound toddler!
Keep in mind that neither of these medications work instantly. It is common to have to wait at least 30 minutes or so before you notice any relief or decreased fever, and for most fevers it can take 90 minutes to get to the full effect.
Milligrams? Milliliters? It can be confusing.
The above charts tell you how many milligrams of each medication your child needs, followed by the milliliters. The doses are based on the child’s weight. The different concentrations can be confusing. Let’s go back to school for a moment for a quick review.
If you take a 500 mg Tylenol tablet, crush it and then dissolve it in a teaspoon (5 ml) of water, you will have 500 mg of Tylenol. If you take the same 500 mg tablet and dissolve it in a cup of water (240 ml). You will still have 500 mg. It is simply in a different concentration.
The first step is to see how many milligrams are appropriate for your child. Your next step is figuring out what volume of fluid will deliver the proper dose. That will depend on the concentration of the medicine.
How to choose
For illness, we don’t have a strong preference between acetaminophen or ibuprofen. Ibuprofen does tend to last a little longer which makes it a good choice for a night dose.
For injury, ibuprofen is a better choice because it is also anti-inflammatory.
One down side is that it can cause tummy upset if given on an empty stomach, especially for repeat doses. This is challenging for sick kids with poor appetites.
Ibuprofen can also inhibit platelet function, thus acting as a blood thinner. Because of this it is typically not used after surgical procedures.
Alternating Dosing
If a fever is lasting longer than a few days in a row, it is worth getting seen by your doctor. If you are dealing with a stubborn fever and have a diagnosis (such as the flu or hand-foot-mouth), it is okay to alternate both of the medications. These are the kids that need help just to be comfortable enough to keep drinking liquids. An example of this would be:
9 am Tylenol
12 noon Advil
3 pm Tylenol (etc…)
If the fever is staying under control, spread out the doses:
9 am Tylenol
1 pm Advil
5 pm Tylenol (etc…)
Dr. Ted’s Tidbit
There are some viruses out there that really send kids over the edge. Hand-foot-mouth disease is usually not so bad, but it has the potential to create so much mouth pain that kids can’t drink any liquids and get dangerously dehydrated. For these kids, when the cause is known and you know they’ll get better with time, I recommend dosing both acetaminophen and ibuprofen simultaneously, just to jumpstart the comfort and help them to drink enough to stay out of the hospital. This shouldn’t be something you’re doing regularly around the clock for days, but for a dose here or there, it’s okay.
Avoid medication errors
Medication errors happen more often than you can imagine. Consider putting a piece of masking tape on the bottles and mark off times and dates of dosages. This can help sleep deprived parents keep track of when they gave what. It also alerts partners if a dose was recently given by another caregiver. This is a good habit with antibiotics as well.
Another option is to keep a notebook nearby and document your doses there. Figure out which method works best for you and make sure that all the caregivers stick with the plan.
Administration strategies
A syringe is worth having on hand. Not only is it more accurate, but it is less likely to spill when your crabby child bats your hand away compared to a teaspoon or medicine cup.
Click this link for a full post full of tips for helping get the medicine down without a battle. It includes a very silly TikTok that Dr. Ted and I did to demo one effective technique
Can you give less than the suggested dose?
When it comes to medicine, some folks want to give as little as possible and try to give partial doses. We understand that instinct. The problem is that sometimes the smaller dose might make a dent, but doesn’t get your child comfortable enough to actually feel better. If you gave a smaller-than-recommended dose, and it only gave a little relief, it’s ok to give the remaining dose to get the full effect. You’d be surprised, we’ve seen instances where the difference between 3.75mL and 5mL is huge in terms of kid outcomes.
In some cases your child might in fact respond to a smaller dose. If that is the case, by all means give the smallest amount that you can get away with. Alas, in our experience, most kids need the full dose to achieve relief.
Are there interactions?
Most of the time, acetaminophen and ibuprofen are safe to give with other medications.
Be careful if you are giving any of the multi-symptom cold remedies (such as DayQuil or NyQuill, which we recommend against anyway). Many of these already have the fever reducer as one of the ingredients; you don’t want to double dose.
Considerations for Young Infants
If your child is under 3 months of age, and you feel that they need any medication, check with your doctor’s office. Any young infant with an elevated temperature needs to be evaluated.
If your child is teething, those symptoms can linger for weeks at a time. Even though they are safe, we try to reserve Tylenol and/or Advil for occasional use. Getting a good night’s sleep if your child is having a ridiculously fussy day seems reasonable once in a while.
For teething, there are many other comfort measures to try first: Teething Blog post
A note on antipyretics for shots
Many parents will ask about giving something Tylenol or Motrin preventatively before or immediately after getting shots. Because there are studies that demonstrate that doing this decreases antibody production to some vaccines, this is not something we universally recommend.
That being said, it’s perfectly acceptable to give something at the first sign of fever or fussiness. This timing will vary from child to child: some kids don’t get fussy for over 8 hours, others will start after 3-6 hours. The only time we recommend doing preventative dosing is if there was a massive fever response to shots previously.
While studies have shown decreased antibody production, most kids still produce enough antibodies to be clinically protected from infection.
However, because we don’t know who will and who will not produce enough, our preference is to play it safe and hold off unless it is needed.
So, if you feel strongly that you want to give preventative dosing regardless, knock yourself out. Be aware that a dose of Tylenol will not impact the actual shot experience. It would be nice, but we promise you it doesn’t.
In summary, middle of the night fevers happen. Everyone should have these medications on hand and stay familiar with the correct doses.






